This is the third in a multi-part series on the effects of the ongoing legalization of marijuana in the worker’s compensation insurance ecosystem. In case you missed them here’s part one, part two and part three. This series is being ran in preparation for a panel on “Legalization of Marijuana and the Impaired Workforce” that the author is moderating at the AmComp Fall Conference in NYC on November 8, 2018. Opinions expressed are those of the author and are not necessarily held by the author’s employer or AmComp. Insurance Nerds readers can save 0 on registering for AmComp with discount code AMCOMPNERDS.
Writing a marijuana prescription to a patient is a relatively recent concept. California, which has had medical marijuana laws in place for two decades, and other similar jurisdictions, have provided access to medical marijuana through doctor recommendations, not prescriptions. These recommendations can be quite lax; and if issued, is really just a blanket approval for a patient to be able to purchase medical pot as they please. This approach, though lackadaisical, was necessary. Marijuana remains federally illegal; technically, providers cannot write a prescription as they get their script-writing power from the Drug Enforcement Agency (DEA) and marijuana has no National Drug Code (NDC).
Presently, there is minimal screening and doctors do little to match specific ailments to prescribed dosage and usage. Physicians have really taken a hands-off approach. This has worked as the current system in one where patients pay out-of-pocket and there is no insurance approval needed. While this may continue to work for general medicinal users, as health insurers are not providing coverage, the same may not hold true for workers’ compensation insurers who have been instructed by states to cover the cost. Requirements around prescriptions, monitoring, and overall patient care would need to transform from the current laissez-faire approach to a heightened level of clinician engagement; however, this shift cannot happen without first fully educating medical providers.
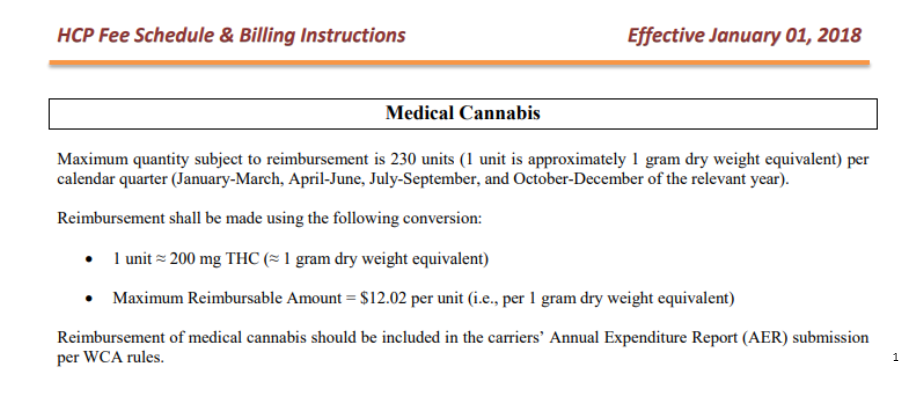
Because of the Controlled Substances Act and the drug’s schedule I classification, there has been minimal research conducted, and information available to physicians is limited. Medical providers do not fully comprehend the full effects nor do they have defined treatment regiments derived from evidence-based medicine. This includes information of what types of marijuana work best for specific ailments and what recommended dosages should be. Even if those circumstances where a prescription is issued rather than a medical card, the script remains a blanket recommendation to obtain marijuana at rate and potency dictated by the patient. The future of cannabis prescriptions, especially under workers’ compensation, should be predicated on care consistent with medical guidelines and supervised closely by the treating physician. The first prerequisite is a qualifying medical condition, followed by guidelines that address the frequency of use, quantity, method of use, and potency.

Proponents of medical marijuana highlight the various types, or strains of marijuana, and the effects each one has for different ailments. However, the learning curve for providers is steep. The number of strains available continues to grow and each promotes itself as unique. Medical providers must accustom themselves to the distinctions that not only advertise benefits it provides (i.e. pain relief, sleep aid, anti-anxiety), but also potency/THC levels and method of consumption. THC levels can vary from less than one-percent to upwards of seventy-percent or more. Methods of consumption include inhalation, ingestion, or transdermal from products including edibles, vape pens, flower, tinctures, oils and patches. Individually, they each produce different reactions and results for patients. Navigating these differences will no doubt be difficult.
Regardless of the challenges ahead, the medical community seems ready to accept the task. Polls from the New England Journal of Medicine and others have ascertained that a majority of physicians would be willing to prescribe medical marijuana. High success rates have been documented among patients suffering from chronic pain, migraines, and post-traumatic stress disorder (especially in US Veterans). Due to these initial studies, most physicians agree there is some role for marijuana is the treatment of certain conditions, though many unknowns remain. A 2014 Medscape poll of clinicians regarding the medical use of marijuana found support among physicians, and about 70% of physicians believed that marijuana had real medical benefits. Yet, the question remains, are they suited to write more than just a generic script? Most patients seem to get more information about attributes and effects from their local ‘budtender’ (someone who serves you at dispensary) that their treating physician. In order to keep some level of professionalism, it should be the other way around. Almost every stakeholder can agree more trials and clinical studies need to be conducted through the research that is required will likely take years to complete. A fair warning has been issues that time is running out. Medical marijuana is here, and available now. It will be important for prescribers to gain information as soon as possible to patients who can benefit from this treatment.
Finally, in addition to treating physicians and pain management specialists, other parties involved in medical decision making need to be educated. This includes not only nurse case managers and medical directors, who work for insurers, but also medical experts involved in independent medical examiners, utilization review, and peer reviews. They too will need a heavy dose of education while working collaboratively with physicians and patients.
Brian Reardon is a Board Member of AmComp and AVP, WC Claims for Maiden Reinsurance. He will be moderating the upcoming panel session on “Legalization of Marijuana and the Impaired Workforce” at the AmComp Fall Conference in NYC on November 8, 2018. Opinions expressed are those of the author and are not necessarily held by the author’s employer or AmComp. Insurance Nerds readers can save 0 on registering for AmComp with discount code AMCOMPNERDS.
About Brian Reardon MBA,ARM,AIS
Brian Reardon, AVP of Worker's Compensation Claims at Maiden Holdings in Bermuda and NYC. He has over 14 years of P&C experience working on all sides of the industry including carrier, reinsurer, TPA, broker and employer. He holds multiple industry designations and a MBA in Insurance and Risk Management from St. John's University. He's a Board Member at AmComp (American Society of Workers Comp Professionals) and a Fellow at the Claims & Litigation Management Alliance.
Brian Reardon, AVP of Worker's Compensation Claims at Maiden Holdings in Bermuda and NYC. He has over 14 years of P&C experience working on all sides of the industry including carrier, reinsurer, TPA, broker and employer. He holds multiple industry designations and a MBA in Insurance and Risk Management from St. John's University. He's a Board Member at AmComp (American Society of Workers Comp Professionals) and a Fellow at the Claims & Litigation Management Alliance.